
The NHS Oversight Framework 2026/27 and what it means for general practice
- Tara Humphrey

- 5 days ago
- 4 min read
At THC, we provide resources for primary care leaders. In this blog, the focus is on the NHS Oversight Framework 2026/27, published on 11th June 2026.
On the face of it, this is a document about NHS trusts and integrated care boards. PCNs are not segmented by it. Practices are not ranked by it. So why should a PCN leader spend any time on it?
Because if you read past the headlines and into Annex B, you find general practice running right through the ICB scorecard.
These are not provider measures. They are the measures by which each ICB will be scored, segmented, and placed in a public league table.
This blog aims to do three things.
Explain how the framework actually works
Set out where general practice sits inside it
Offers a view on what that shift means for the way ICBs will engage with general practice over the coming year.
The policy sequence
The Oversight Framework is not a standalone release. It is the accountability layer beneath the new NHS operating model set out in the 10 Year Health Plan, and it sits alongside the Medium Term Planning Framework, the Strategic Commissioning Framework, and the forthcoming Model ICB Blueprint.

The 10 Year Health Plan set the ambition through its three shifts, hospital to community, analogue to digital, sickness to prevention.
The Oversight Framework is the mechanism that decides what happens when an organisation delivers against that ambition, and what happens when it does not.
It is deliberately evolutionary. NHS England has kept the core architecture from the 2025/26 framework rather than rebuilding it.
The notable changes this year are that ICBs and providers are now segmented on an aligned basis; the methodology has moved from a quartile approach to statistical thresholds; there are new metrics for mental health, community, and ambulance trusts; and there is clearer recognition of high performers through advanced foundation trust status. This is a refinement of a system that is now bedding in, not a fresh start.
How the 3 mechanisms work
Delivery segmentation. Every ICB and provider is given a segment from 1 to 4.
Segment 1 means the organisation performs highly with only a narrow range of issues.
Segment 4 means it performs significantly below average across a range of areas and is likely to need a coordinated response and possible intervention. Segments are calculated from scored metrics, benchmarked nationally, and refreshed every quarter.
There is one override worth knowing. Any organisation in financial deficit is automatically prevented from sitting in segment 1 or 2 until that deficit is resolved.

Capability assessment. Separately, each organisation is rated on leadership, governance and the ability to improve, from green, through amber green and amber to red.
Where segmentation asks what an organisation has delivered, capability asks whether it has the capacity to put things right.
Oversight response. The two are then combined.
Strong delivery and high capability earn lighter-touch oversight and access to freedoms, including advanced foundation trust status and capital flexibilities.
Weak delivery and low capability attract the most intensive scrutiny, mandated support, enforcement powers, and restrictions on very senior managers' pay.
Segments and capability ratings are published, including public league tables, so organisations and the public can see where everyone stands.
Primary Care Networks are not named, but primary care is scored
The framework applies to ICBs and providers as statutory bodies.
It does not segment PCNs or individual practices.
But it states plainly that ICBs are responsible for primary care commissioning and population health, and that how effectively an ICB commissions, assures and oversees primary care forms part of its oversight, through annual assessments and future capability assessments.
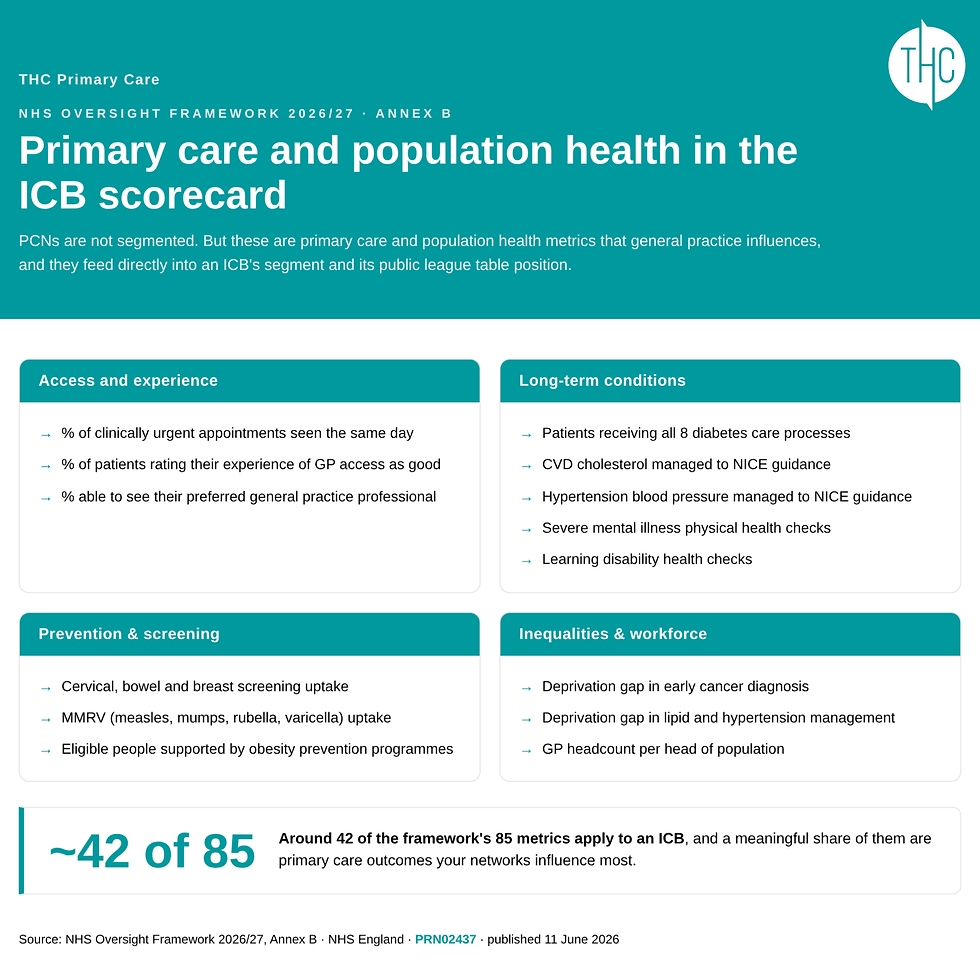
Among the measures that determine an ICB's segment are the percentage of clinically urgent appointments that happen on the same day, the percentage of patients rating their experience of GP access as good, and the percentage able to see their preferred general practice professional.
They include diabetes care processes; cholesterol and blood pressure management to NICE guidance; severe mental illness and learning disability health checks; cervical, bowel, and breast screening uptake; smoking in pregnancy; GP headcount per head of population; and deprivation gaps in early cancer diagnosis and in lipid and hypertension management.
Of the 85 metrics in the framework, an ICB is assessed against around 42, and a meaningful share of them are primary care outcomes.
The accountability chain

NHS England remains ultimately accountable for the primary care commissioning it has delegated to ICBs, and it holds ICBs to account for that performance through delegation agreements.
During 2026/27, NHS England will work with ICBs to develop a capability assessment that explicitly reflects their role as strategic commissioners, including for primary care, in alignment with the neighbourhood health strategy.
From 2027/28, formal ICB capability assessments are expected to be folded into the annual assessment, alongside a delivery score derived from the ICB's average segment.
There is also a structured development offer in 2026/27 to strengthen ICB commissioning capability and the use of commissioning levers to support neighbourhood health.
Confirmed, new and open
Confirmed | New | Open |
The segmentation, capability and oversight response architecture continues from 2025/26 | ICB delivery segmentation is now aligned with providers, using statistical thresholds rather than quartiles | The detailed methodology for the future ICB capability assessment |
ICBs are accountable for primary care commissioning, with NHS England holding them to account via delegation | A formal ICB capability assessment covering the strategic commissioning role, including primary care, to be developed in 2026/27 | How heavily primary care performance is weighted within the ICB score |
Public league tables and a transparent dashboard | The financial deficit override that blocks segment 1 or 2 | How ICB accountability cascades into PCN and practice level conversations |
What this means for PCN leaders now
These are the measures your ICB will be watching, because they feed its own score and its place in the league table.
So... if your ICB comes directly to your PCN or to your practices to look at same-day access, long-term condition management, or screening uptake, you now understand why.
About us
THC Primary Care is an award-winning healthcare consultancy specialising in Primary Care Network management and the creator of The Business of Healthcare. With over 20 years in the industry, we have supported more than 300 PCNs through interim management, training and consultancy.
Our expertise spans project management and business development across both primary and public sectors. Our work has been published in the London Journal of Primary Care, and we have authored over 250 blog posts sharing insights on primary care networks.
Keep in Touch






.png)
